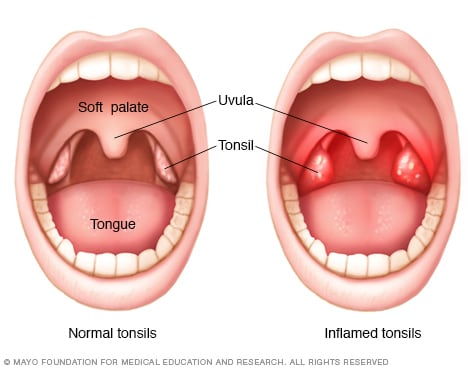
On Wednesday (6/1/22), I shadowed Dr. Bloedon and other surgeons. There were not many surgeries scheduled on that day but I did get to watch tonsils being removed and parts of the nose being repaired to help breathing. Also, I should note that the last surgery was stopped due and rescheduled to another day due to the patients heart beat being irregular (flutters and speeds up and down).
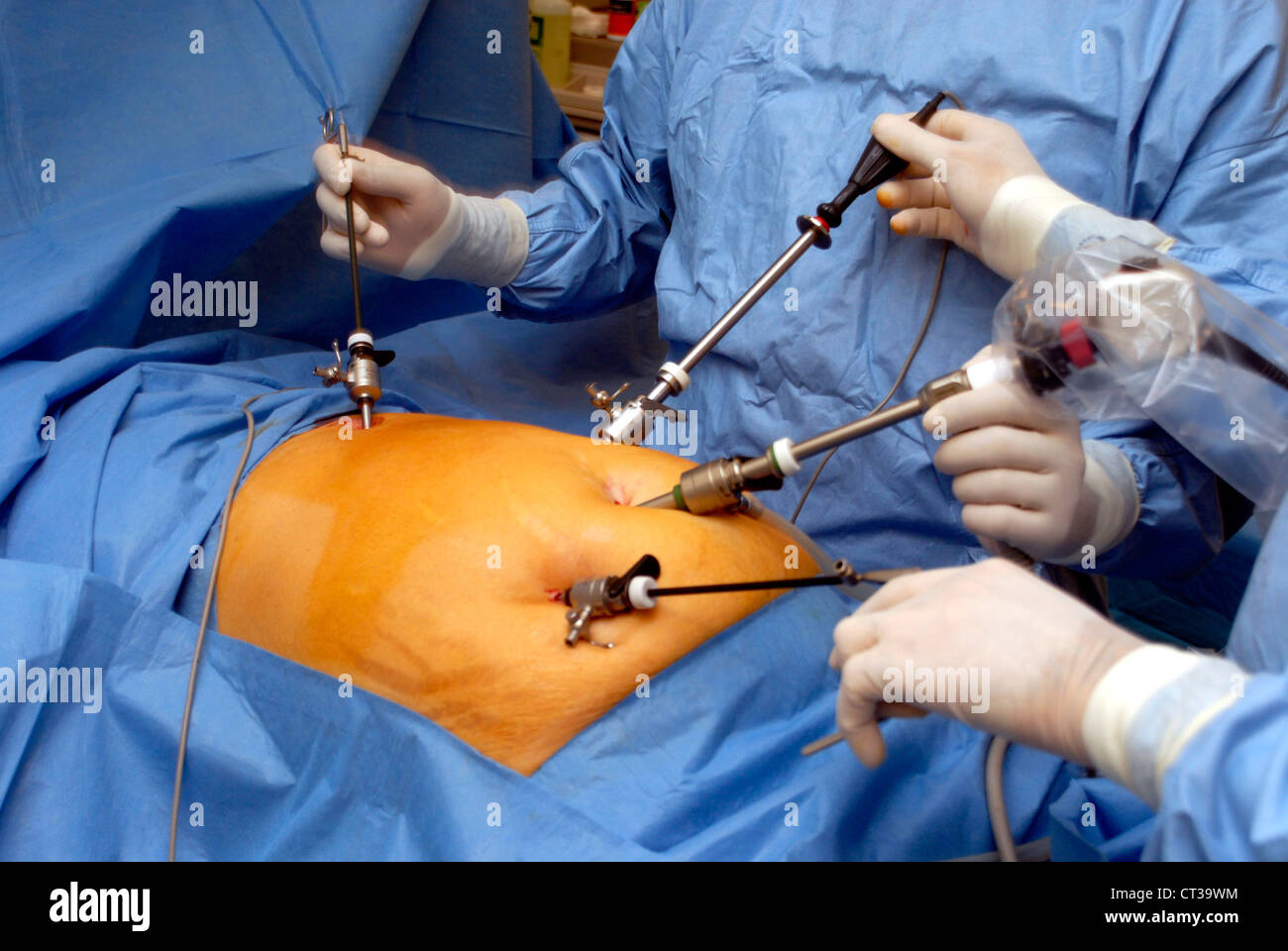
On Tuesday (5/24/22), I met with Dr. Dorfman and many of his colleagues and observed first hand many different types of surgeries. I put scrubs on for the first time and saw surgery up close for the first time as well. While observing the surgeons, I saw many tube surgeries on small kids (for ear infections), an ankle fracture surgery, and also a gallbladder removal. The gallbladder removal was my favorite as they have a non-invasive technique to take it out. In short, they fill up the stomach with a gas and then make a few holes in the stomach to carefully burn the gallbladder and separate it from the other internal organs (use screen to navigate through body).
Today was a great day in the OR! I was back in the Raleigh Orthopedic Surgery Center and saw 5 surgeries today: a tendon repair using an artificial tendon, an ankle fusion, a broken ankle, multiple toe realignments, and a tendon cleanup.
One of the most interesting things that I saw today was arthroscopy being used twice in two different surgeries. Arthroscopy is where a probe with a camera is used and inserted into the body, so the surgeon can see what he/she is working on without having to make a big incision. Dr. Logel used arthroscopy today in the ankle joints of both patients. They both had had past injuries which caused debris, also known as scar tissue, cartilage, etc., to form in between the two bones. This causes inflammation of the joint and the patients feel pain. To get rid of this debris, Dr. Logel made two very small incisions on the joint and put the camera probe in on one side and a vibrating tool in the other. He would use the camera screen to see where his tool was and would cut away at all of the debris. He said arthroscopy was the doctor’s videogame, and he was pretty good at it! I enjoyed this part of surgery because I could fully see what was going on during the surgery, rather than just seeing from farther away.
Another cool thing that I saw today was a patient whos ankle joint had no cartilage in it between the two bones that she had minimal motion of the ankle and lots of pain as the bones were constantly rubbing together. The surgery that was done for this patient was to fuse the two ankle bones together. This was done by removing any debris from the joint, breaking a bit of bone here and there to simulate a bone break (the bone heals faster if it is broken), and then putting 4 screws in to the two bones to lock it together. Dr. Logel explained how the patient would still have some ankle motion from side to side but the ankle wouldn’t be able to move up and down. However, this was only a little less movement than she had already been dealing with, just without the pain.
Lastly, another thing that I thought was very interesting was the way that Dr. Logel fixed a broken ankle. This patient had broken his ankle 3 weeks prior and it had already started forming bone callus, but it wasn’t aligned correctly. This said, Dr. Logel went into the ankle and basically rebroke the ankle, taking out all of the newly formed bone callus and anything that was holding the bone sections together. He then used a tight clamp and an x-ray called the “C Arm” to make sure that the bones were lined up correctly and then he drilled a 7 screw plate into his ankle, securing the bones from separating.
Overall, I am very appreciative and grateful that I was given the opportunity to go into the OR with Dr. Logel and see about 10 surgeries! Everyone in the OR was very friendly, welcoming, and eager that someone was interested in their field! I learned so much more than I ever could have just in clinic and it was great to actually see things being fixed in person!
The Surgery room setupThe staff lounge room – had to have some caffeine because surgery makes you tired!Waiting to go into surgery!All the rooms use x-rays, so you have to wear lead dresses and neck protectors (how cute!)
What an experience! Today I started my day bright and early at 7 AM in the Surgery center of the Raleigh Orthopedic Clinic. I scrubbed in and was on my way to the first surgery! All of the nurses were so nice and helpful, showing me the ins and outs of the OR from how to put on your mask to what you can and can’t touch. Everything in the operating room is very sterile, so I had to make sure that I was far enough away from contaminating anything.
The first surgery was an accessory bone removal in the top of the foot. I expected to feel nauseous or queasy observing the surgery, but I surprised my self and felt fine! During this surgery, Dr. Logel walked me through the steps he was taking, including how he almost chipped away at the bone until it popped out. He had to make sure that he didn’t cut into or break any ligaments or veins, so he was very cautious of where he was working. It was cool to see the bone on the table after the surgery and to understand how such a small bone could be causing such tremendous pain.
The second surgery that I saw today was a patient who fell and broke her ankle. Dr. Logel showed me the x-rays and you could not only see the crack in the bone, but you could also see how the tendon in between the bones was moved and caused the tibia and fibula to be separated. During this surgery, Dr. Logel drilled plates and screws into the bone to fix the crack and then used what they call “tight rope” to pull the two bones together over the tendon. The tight rope was basically a very small, but strong string that was anchored into the sides of the bone and pulled very tightly together. The operating room uses a portable x-ray machine during the surgery which was very interesting to watch because Dr. Logel would use it to make sure his drill or screws were in the right spot of the bone where he couldn’t see.
The next surgery that we went to was a patient who had very bad arthritis in the 1-2 tarsal- metatarsal joints due to an injury a few years earlier. The procedure that Dr. Logel did on this patient was a joint fusion, which is where they fuse the two bones together, so there isn’t a joint anymore. This was on the top of the foot, so the skin was very thin and there were a lot of little veins that Dr. Logel had to work around. The procedure for this surgery was to clean out the joints of any excess cartilage and chip off any excess bone so they two bones could come together evenly. It was interesting to watch this part of the surgery because I didn’t know that bone was so easily chipped away with certain tools. After Dr. Logel cleaned out the joints, he put 5 screws into the top and sides of the foot to hold the bones together, so they could start growing together. This is what happens when a bone is broken; the bone realizes there’s a crack and starts to reform bone.
The last surgery of the day was by far my favorite surgery. This patient had ruptured his Achilles tendon and this surgery was to repair it. Before the surgery, Dr. Logel showed me how you can tell if the Achilles is torn by the alignment of the foot neutrally and if you press on the calf, if the toes move. It was interesting to see the difference between this patient’s normal and ruptured tendons. The procedure of this surgery was to take out the frayed and ruptured parts of the tendons, and then finding the other two sides of the tendon and connecting them together. This was done by putting many stiches into each side with thick string and then yanking on both sides of the tendon to pull them together. It was so fascinating to see how you can still use what is left of your tendon to fill in the missing spots. Dr. Logel then used disintegrating stiches to hold the new tendon together, allowing the tendon to grow and reform over the stiches. Shockingly, this was the fastest surgery and only took a few minutes to do the actual procedure.
Overall, I had a very busy but fascinating day in the operating room and it was crazy to see the life behind the clinic!