I’ve had an incredible journey with Dr. Lawal, and to be frank, I’m not ready to let it go. Dr. Lawal has been absolutely genial to not only me but also his patients and faculty – no matter how busy he is, Dr. Lawal makes the constant sacrifice to help his own surroundings before helping himself, and there’s more than meets the eye. I could not be more grateful for this experience!
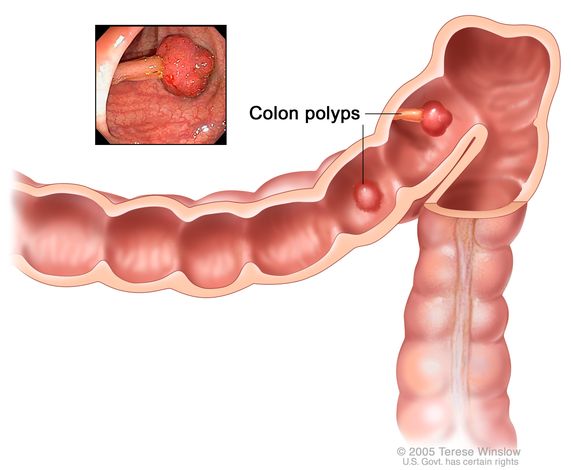
I’ve continued to develop strong relationships with Dr. Lawal’s patients, most of whom have been building acid reflux and colorectal cancers. Acid reflux is a very common chronic digestive disease that causes stomach acids/liquid bile to travel through the esophagus, otherwise known as the food pipe – chest pains and regurgitation of consumed substances occur directly from this abnormal movement.
Unfortunately, one common pattern I discovered among the patients is that they typically consume foods right before sleeping; in other words, they ‘snack’ prior to heading off to bed without the necessary digestion. Dr. Lawal explicated that substances should be decomposed within a 2-3 hour limit to alleviate reflux. The same instance can also be applied to the consumption of medication; taking medications prior to sleeping will result in colorectal damage, creating ulcers.

Dr. Lawal also lectured me on the plethora of gastric diseases that remain active in adulthood, most notably, diverticulosis. The diverticular disease pushes out the weaker portions of the colon to create small pouches, or ‘pockets,’ across the linning. Subsequently, small fragments of undigested food get stuck in these pockets, yielding gastric inflammation.
One other viral infection is hepatitis, which attacks the liver and also creates inflammation. Among five patients, one contracted Hepatitis-C (there are also A, B, D, and E), which leads to abdominal pain, internal bleeding, and fatigue. According to Dr. Lawal, 30% of men and 20% of women contract this disease.
I’m really excited (and a bit sad) for tomorrow! Looking forward to seeing Dr. Lawal and, hopefully, more patients to interact with. Gastroenterology may now be one of my favorite medical studies 🙂
– Nishant



/GettyImages-1141295436-4f52fbde72b14ee8bd7660e29be326ce.jpg)